





Despite a notable decrease in HIV/AIDS prevalence in Burundi, stigmatization persists
By Avit Ndayiziga
Even though HIV/AIDS prevalence has significantly declined on a global scale, stigma and discrimination remain significant obstacles in achieving the 95-95-95 UNAIDS targets aimed at ending HIV as a public health emergency by 2025.
This message was echoed by Angeli Achrekar, Deputy Executive Director of the Programme Branch at the Joint United Nations Programme on HIV/AIDS and an Assistant Secretary-General of the United Nations during the 12th International AIDS Conference held in Brisbane, Australia this past July.

In Burundi, as elsewhere in the world, HIV/AIDS prevalence has significantly declined. It decreased from 5.3% in 1993 to 1% in 2022 in Burundi. However, HIV/AIDS stigma remains a hushed reality on the ground among people living with HIV/AIDS (PLWHA).
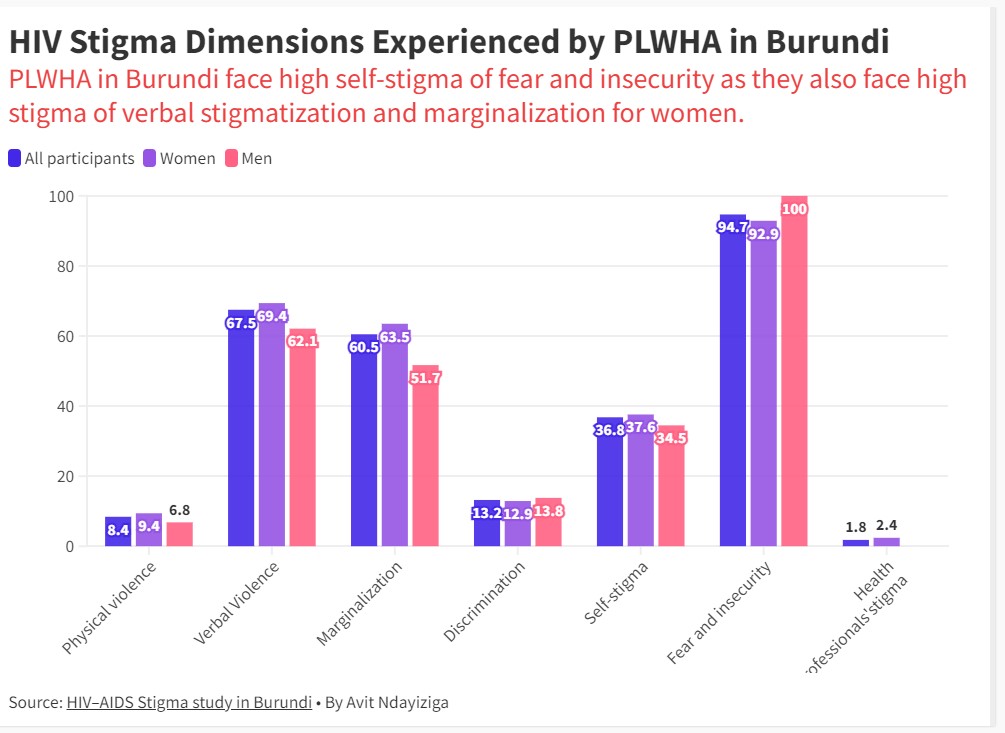
According to the HIV–AIDS Stigma study in Burundi, 41.8% of people living with HIV/AIDS (PLWHA) face discrimination, with women accounting for 46.9% and 57.2% experiencing self-stigma, in other words, they feel sorry or bad for themselves.
As per the same study, HIV/AIDS-related stigma is currently a severe problem among AIDS patients globally, Africa, Burundi included. Stigma has implications for the health and well-being of PLWHA on many levels, causing psychological problems such as depression, low self-esteem, stress, and even suicidal ideation.
Moreover, fear of discovery of HIV status leads PLWHA to hide their seropositivity, making it difficult to treat the disease, as stigma has also been associated with non-adherence to ART.
Victims express their resentment
Niyonsaba Mariam is a flood survivor from Gatumba in the eastern part of Bujumbura, the economic city of Burundi, and lives with HIV/AIDS in Sobel camp, one of three sites that host people displaced by floods and landslides three years ago. She was diagnosed with HIV/AIDS two years ago.

“The first time I witnessed discrimination was when the mother of a child who was playing with my son told him not to hurt him because HIV could be transmitted to his son. Another incident occurred when I tried to borrow a knife from my neighbor, but they refused. They insisted that I should buy my own knife,” says Mariam.
Mukeshimana Jeannette, a widow who has been living with HIV for seven years, adds that at school her son was discriminated against to the point that he wanted to drop out of school.
“I had to go to the school and request the teacher to ensure that my son would never be discriminated against by his classmates. Otherwise, he had started thinking of quitting. Furthermore, our neighbors also caution their children to be vigilant when playing near our home and use our utensils, “Jeannette added.
Ndikuriyo Amani, a 22-year-old woman with one child, says that her dispute with her husband led the neighborhood to know about her HIV status.
“After enduring an illness and being hospitalized for several months, I finally began taking ART medicines. However, I had kept this information hidden from my husband out of shyness. This provoked my husband to react irrationally and insist on divorcing me, questioning where I could have contracted HIV from. Our relationship became entangled in constant disputes until our families intervened and arranged a meeting to reconcile us. The news of my status spread throughout the neighborhood, causing further complications. Being born with HIV has instilled in me everlasting resentment toward my parents for not protecting me,” Amani explained.
Antolie 52, a community agent who is HIV positive says how curing the unknown disease caused her to sell all her possessions. However, it led her to community advocacy to raise awareness within the community.
“I sold all my properties paying a witch thinking that my husband was bewitched since he was sick for many months. As his health condition did not improve, our neighbors advised us to go to the hospital. We went to the hospital and were diagnosed with HIV/AIDS, which shocked me,” says Anatolie.
As Anatolie continued, “Despite the ongoing gossip behind our backs, it is crucial to educate people on how to treat HIV-positive individuals with respect. Therefore, as a community agent, I took it upon myself to visit households and openly disclose my own HIV status, while also teaching them about proper treatment of those living with the virus. This approach has proven effective in preventing discrimination,” Anatolie concluded.
Data backs the presence of stigma and discrimination in Burundi
The HIV–AIDS Stigma study in Burundi, with the support of USAID, revealed that 41.8% of individuals living with HIV in Burundi face discrimination, while 57.2% experience self-stigmatization.
The same study conducted back in 2014 also reported high rates of stigmatization, with 68% of participants having experienced it at least once and 84.9% reporting episodes of self-stigma. Self-stigma affects 86.9% of Women compared to men at 79.9%.
Although there has been some progress, current data indicates that stigma continues to significantly impact the HIV epidemic and access to services for vulnerable populations.
Hamza Venant Burikukiye, the General Director of Capes+ (a collection of associations for people living with HIV/AIDS), acknowledges that some progress has been made in reducing the HIV/AIDS-related stigma. However, he laments that there is still a long way to go.

“Among 41.8% of individuals living with HIV in Burundi facing discrimination, it is sad that 24.1% face discrimination that comes from associations and centers in charge of HIV/AIDS services providing,” says Hamza. He adds that this response fuels anger among PLWHA since they did not become infected on purpose
According to him, HIV/AIDS stigma is caused by many issues including poverty because it can be a means to an end.
“At centers in charge of HIV/AIDS services providing, services providers want to make a profit from HIV/AIDS. For instance, if today, it happens that HIV/AIDS vaccination is found, these people will lose their jobs. This is the reason why they keep pushing back PLWHA. How is it possible that an HIV/AIDS-negative person is the one who speaks on our behalf, and leads an HIV/AIDS-related project? Venant asked. They want us to stay beggars. Due to this HIV/AIDS services providers are more discriminatory than the community we live in,” Venant explained.
Although significant progress has been made in eliminating stigma in Burundi, Burikukiye says that the fight against HIV stigma in this country is far
from over. Interventions at the interpersonal and community level should be promoted. Likewise, at a structural level, it would be instrumental to use the media to create collective awareness about this issue.
The UNAIDS official confirms stigma and discrimination among PLWHA
During the IAS 2023, the 12th IAS Conference on HIV Science held in Brisbane, Australia from 23-26 July,20223, in a symposium session focussing on 95-95-95 targets aimed at ending HIV as a public health emergency Achrekar stressed the Scaling up ART in low-middle-income countries. However, the UNAIDS official confirmed that stigma and discrimination undermine HIV prevention and treatment programs.
“In 54 countries, 59% of people had discriminatory attitudes towards people living with HIV. That is six times higher than the 2025 global target. In 13 countries, more than 75% of those surveyed reported discriminatory attitudes.
People living with HIV who anticipate high levels of stigma are 2.4 times more likely to delay enrollment in care until they are very ill,” Achrekar concluded.
The UNAIDS official emphasized that addressing stigma and discrimination requires a multi-level framework that creates an inclusive environment for people living with HIV/AIDS (PLWHA).

The IAS 2023, the 12th IAS Conference on HIV Science highlighted that in 2022, a total of 1,300,000.0 new HIV infections worldwide were reported, with 630,000 deaths among the 39 million People Living With HIV/AIDS. Sub-Saharan Africa is home to approximately two-thirds (67%) of the global HIV population and also accounts for two-thirds of the new HIV infections. Additionally, in that same year, a total of $20.8 billion was allocated toward HIV programs in low and middle-income countries.
This story was supported by the Internews Health Journalism Network.

